Herniated Disc
Herniated Disc
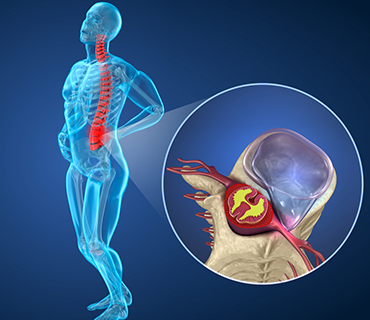
The bones (vertebrae) that form the spine in your back are cushioned by small discs. These discs are round and flat, with a tough, outer layer (annulus) that surrounds a jellylike material called the nucleus. Located between each of your vertebra in the spinal column, discs act as shock absorbers for the spinal bones. Thick ligaments attached to the vertebrae hold the pulpy disc material in place.
A herniated disc (also called a slipped or ruptured) disc is a fragment of the disc nucleus that is pushed out of the annulus, into the spinal canal through a tear or rupture. Discs that become herniated usually are in an early stage of degeneration. The spinal canal has limited space, which is inadequate for the spinal nerve and the displaced herniated disc fragment. Due to this displacement, the disc presses on spinal nerves, often producing pain, which may be severe.
Herniated discs can occur in any part of the spine. Herniated discs are more common in the lower back (lumbar spine), but also occur in the neck (cervical spine). The area in which you experience pain depends on what part of the spine is affected.
Causes: A single excessive strain or injury may cause a herniated disc. However, disc material degenerates naturally as you age, and the ligaments that hold it in place begin to weaken. As this degeneration progresses, a relatively minor strain or twisting movement can cause a disc to rupture.
Certain individuals may be more vulnerable to disc problems and, as a result, may suffer herniated discs in several places along the spine. Research has shown that a predisposition for herniated discs may exist in families, with several members affected.
Herniated Disc Symptoms:
Symptoms vary greatly depending on the position of the herniated disc and the size of the herniation. If the herniated disc is not pressing on a nerve, you may experience a low backache or no pain at all. If it is pressing on a nerve, there may be pain, numbness or weakness in the area of the body to which the nerve travels. Typically, a herniated disc is preceded by an episode of low back pain or a long history of intermittent episodes of low back pain.
Lumbar spine (lower back): Sciatica frequently results from a herniated disc in the lower back. Pressure on one or several nerves that contribute to the sciatic nerve can cause pain, burning, tingling, and numbness that radiates from the buttock into the leg and sometimes into the foot. Usually one side (left or right) is affected. This pain often is described as sharp and electric shock-like. It may be more severe with standing, walking or sitting. Along with leg pain, you may experience low back pain.
Cervical spine (neck): Symptoms may include dull or sharp pain in the neck or between the shoulder blades, pain that radiates down the arm to the hand or fingers, or numbness or tingling in the shoulder or arm. The pain may increase with certain positions or movements of the neck.
Diagnosis :
Diagnosis is made by a neuro-specialist based on your history, symptoms, a physical examination and results of tests, including the following:
- X-ray: Show the structure of the vertebrae and the outline of the joints. X-rays of the spine are obtained to search for other potential causes of pain, i.e. tumors, infections, fractures, etc.
- Magnetic resonance imaging (MRI): A diagnostic test that produces 3-D images of body structures using powerful magnets and computer technology; can show the spinal cord, nerve roots and surrounding areas, as well as enlargement, degeneration, and tumors.
- Electromyogram and Nerve Conduction Studies (EMG/NCS): These tests measure the electrical impulse along nerve roots, peripheral nerves and muscle tissue. This will indicate whether there is ongoing nerve damage, if the nerves are in a state of healing from a past injury or whether there is another site of nerve compression.
Treatment: Fortunately, the majority of herniated discs do not require surgery. However, a very small percentage of people with herniated, degenerated discs may experience symptomatic or severe and incapacitating low back pain, which significantly affects their daily life.
The initial treatment for a herniated disc usually is conservative and medical management. Your doctor may prescribe bed rest or advise you to maintain a low, painless activity level for a few days to several weeks. This helps the spinal nerve inflammation to decrease.
A herniated disc frequently is treated with nonsteroidal anti-inflammatory medication if the pain is only mild to moderate. An epidural steroid injection may be performed utilizing a spinal needle under X-ray guidance to direct the medication to the exact level of the disc herniation.
Your doctor may recommend physiotherapy. The therapist will perform an in-depth evaluation, which, combined with the doctor’s diagnosis, will dictate a treatment specifically designed for patients with herniated discs. Therapy may include pelvic traction, gentle massage, ice and heat therapy, ultrasound, electrical muscle stimulation, and stretching exercises. Pain medication and muscle relaxants also may be beneficial in conjunction with physical therapy.
Surgery: Doctor may recommend surgery if conservative treatment options, such as physiotherapy and medications, do not reduce or end the pain or increase in severity of pain. He will talk to you about the types of spinal surgery available and, depending on your specific case, will help to determine what procedure might be an appropriate treatment for you. As with any surgery, a patient’s age, overall health and other issues are taken into consideration when surgery is considered.
You may be considered a candidate for spinal surgery if:
- Back and leg pain limits normal activity or impairs your quality of life
- You develop progressive neurological deficits, such as leg weakness and/or numbness
- You experience loss of normal bowel and bladder functions
- You have difficulty standing or walking
- Medication and physical therapy are ineffective
- You are in reasonably good health
Surgical Terms: Artificial disc surgery — Surgical replacement of a diseased or herniated lumbar disc with a manufactured disc. The artificial disc consists of a plastic core between two chrome plates that lock into the spine. The PRODISC-L is an artificial intervertebral disc made from metal and plastic that is used to treat pain associated with degenerative disc disease (DDD).
Discectomy — Surgical removal or partial removal of an intervertebral disc.
Laminectomy — Surgical removal of most of the bony arch, or lamina of a vertebra.
Laminotomy — An opening made in a lamina, to relieve pressure on the nerve roots.
Spinal Fusion — A procedure in which bone is grafted onto the spine, creating a solid union between two or more vertebrae; and in which instrumentation such as screws and rods may be used to provide additional spinal support.
Lumbar Spine Surgery: Lumbar laminotomy is a procedure often utilized to relieve leg pain and sciatica caused by a herniated disc. It is performed through an incision down the center of the back over the area of the herniated disc. During this procedure, a portion of the lamina may be removed. Once the incision is made through the skin, the muscles are moved to the side so that the surgeon can see the back of the vertebrae. A small opening is made between the two vertebrae to gain access to the herniated disc. After the disc is removed through a discectomy, the spine must be stabilized. Spinal fusion often is performed in conjunction with a laminotomy. In more involved cases, a laminectomy may be performed.
Cervical Spine Surgery:
The medical decision to perform the operation from the front of the neck (anterior). After the disc is removed, the spine often needs to be stabilized. This is accomplished using a cervical plate and screws (instrumentation), and, often, spinal fusion.
Post surgery: Your doctor will give you specific instructions post-surgery and usually prescribe pain medication. He or she will help determine when you can resume normal activities such as returning to work, driving and exercising. Some patients may benefit from supervised rehabilitation or physical therapy after surgery. Discomfort is expected while you gradually return to normal activity, but pain is a warning signal that you might need to slow down.
Prevention Tips: Once you have recovered from surgery and checked with your doctor, you may resume moderate exercise. The following tips may be helpful in preventing low back pain and herniated discs.
- Do crunches and other abdominal-muscle strengthening exercises to provide more spine stability. Swimming, stationary bicycling and brisk walking are good aerobic exercises that generally do not put extra stress on your back.
- Use correct lifting and moving techniques, such as squatting to lift a heavy object. Don’t bend and lift. Get help if an object is too heavy or awkward.
- Maintain correct posture when you’re sitting and standing.
- If you smoke, quit. Smoking is a risk factor for artherosclerosis (hardening of the arteries), which can cause lower back pain and degenerative disc disorders.
- Avoid stressful situations if possible, as this can cause muscle tension.
- Maintain a healthy weight. Extra weight, especially around the midsection, can put strain on your lower back.